Published: May 20, 2026
Amogh Nootigattu
Independent Research Article
In 1932, the U.S. Public Health Service enrolled 399 Black men in a syphilis study and deliberately withheld treatment for forty years. Nearly a century later, a quieter form of medical exclusion is being encoded into the algorithms that scan living brains, this time dressed in the language of machine learning and statistical confidence.
Artificial intelligence is transforming neurological diagnostics with a speed that outpaces both regulation and ethical scrutiny. Deep learning algorithms now analyze MRI and CT scans to detect conditions ranging from Alzheimer’s disease to multiple sclerosis with accuracy rates that rival, and in narrow tasks surpass, human specialists (Rezaei et al., 2024). These tools promise to extend expert-level care to underserved clinics, rural hospitals, and low-resource settings where a neurologist may be days away. Yet a growing body of evidence reveals a foundational flaw in how these systems are built: the datasets that train them are profoundly homogeneous, and that homogeneity produces diagnostic tools that systematically fail the patients they were meant to serve.
To understand why algorithmic bias emerges in neurological AI, it is necessary to understand how these systems are trained. Most modern diagnostic tools rely on supervised machine learning: an algorithm learns to identify disease-related patterns, including subtle changes in cortical thickness, hippocampal volume, and white matter integrity, by studying thousands of labeled brain scans. It applies those learned associations to new patients. The problem begins with the data.
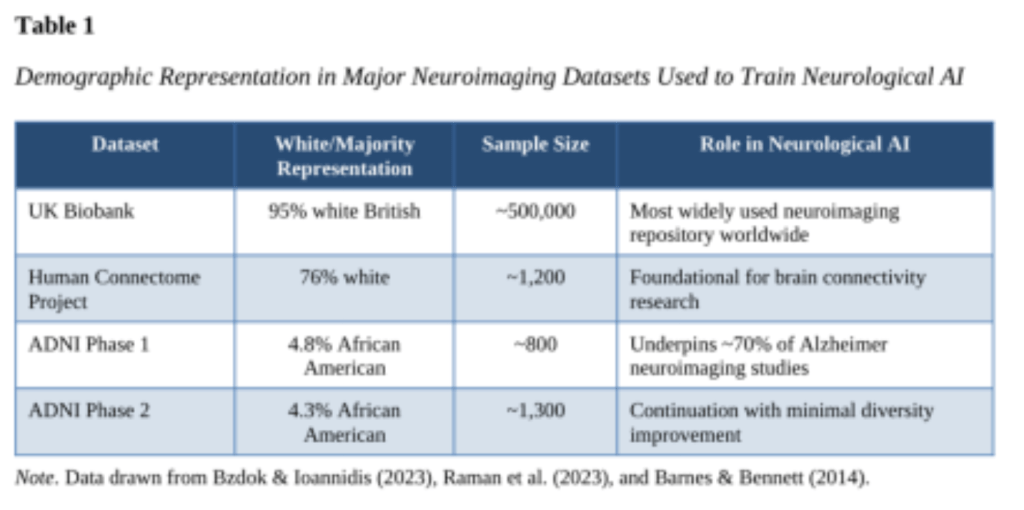
The UK Biobank, one of the most widely used neuroimaging repositories worldwide, draws 95 percent of its participants from white British populations, with the Human Connectome Project similarly dominated at 76 percent white (Bzdok & Ioannidis, 2023). The Alzheimer’s Disease Neuroimaging Initiative (ADNI), whose data underpins roughly 70 percent of indirect Alzheimer’s neuroimaging studies, enrolled only 4.8 percent African American participants in its first phase and 4.3 percent in its second (Raman et al., 2023; Barnes & Bennett, 2014). When a model learns what healthy or diseased brain structure looks like almost exclusively from one demographic, its internal representation of neurological normality becomes a portrait of that group, not of the human species.
This matters because brain anatomy varies meaningfully across populations. Research comparing white and African American participants has documented volumetric differences in subcortical structures, cortical thickness, and surface area across frontal, parietal, temporal, and occipital regions (Cano et al., 2024). A landmark 2022 study in Science Advances by Li et al. tested fMRI-based behavioral prediction models across racial groups and found that when models were trained on data dominated by white Americans, prediction errors were systematically higher for African Americans, with the bias directly traceable to the demographic skew of the training data (Li et al., 2022). An algorithm that has never seen a demographically representative brain cannot reliably read one.
These representational failures have direct consequences for patients. Early detection of Alzheimer’s disease allows patients to access disease-modifying therapies, participate in clinical trials, and make informed decisions while cognitive clarity remains. A false negative closes that window permanently. A false positive triggers unnecessary interventions, psychological harm, financial burden, and discrimination in insurance and employment. Both error types are more likely in underrepresented groups when training bias goes unaddressed.
Adjacent fields confirm the pattern. A Stanford-led study creating the Diverse Dermatology Images dataset found that state-of-the-art dermatology AI models performed substantially worse on dark skin tones, with sensitivity as high as 0.69 for lighter skin but as low as 0.23 for darker skin, a nearly three-fold disparity (Daneshjou et al., 2022). When models were fine-tuned on diverse data, the performance gap closed, demonstrating that the bias is not an inherent limitation of AI. There is no principled reason why neurological diagnostic AI is immune to the same dynamics; the complexity of three-dimensional brain imaging may, in fact, make demographic generalization harder, not easier. The regulatory picture deepens the concern: a 2024 scoping review of 692 FDA-approved AI medical devices found that only 3.6 percent reported race or ethnicity data, 99.1 percent provided no socioeconomic data, and 81.6 percent did not report the age of study subjects (Ong et al., 2024). Neurological AI tools can reach clinical deployment with almost no public accountability for their demographic performance.
What makes this an ethical crisis rather than merely a technical inconvenience is that it does not arise in a vacuum. It reflects and amplifies existing disparities in who has historically received quality neurological care. Communities of color and rural patients have long faced structural barriers to specialist care. Neurological AI was introduced partly to dismantle those barriers. But when the tools themselves are trained on data that excludes these communities, they do not democratize access. They automate exclusion. They take historical disparities in care, encode them into training data, and deploy that encoded inequality as though it were objective medical truth.
This raises a deeper neuroethical concern about consent and data governance. Patients whose brain scans contribute to training datasets may not understand, and likely have not explicitly agreed, that their data will be used to build systems that disproportionately serve other populations. The communities most underrepresented in training data are often those with the most historical reason to distrust medical institutions. As Bzdok and Ioannidis (2023) note in Nature Neuroscience, the very methods of neuroscience, including how researchers recruit, how they build atlases, and how they define normative anatomy, can inadvertently exclude minorities and yield biased brain-behavior relationships. Diversity commitments without structural accountability reproduce the same inequities they claim to address.
The standard policy response to training bias calls for more diverse datasets, disaggregated accuracy metrics, and community oversight. These are necessary but insufficient on their own. What the field requires is a structural mechanism that makes diverse representation technically feasible, legally protected, and institutionally enforced simultaneously. I propose a framework I term Federated Equity Architecture (FEA), drawing on three converging developments in the research literature.
The first component is federated learning as the default training paradigm for neurological AI. Federated learning allows a model to train across multiple institutions, including community health centers, tribal hospitals, and historically Black university medical programs, without centralizing or sharing raw patient data (Li et al., 2020; Dinsdale et al., 2022). Each site trains locally and shares only model gradients with a central coordinator. This resolves the core obstacle to diverse data collection: the privacy laws (HIPAA, GDPR) that make centralized multi-institutional neuroimaging databases legally fraught for underserved community clinics, which often lack the infrastructure to participate in conventional data-sharing agreements. Federated learning decouples participation from data transfer.
The second component is mandatory disaggregated performance certification as a prerequisite for FDA clearance. Currently, only 3.6 percent of FDA-approved AI medical devices report racial or ethnic performance data (Ong et al., 2024). This must become a hard requirement. Specifically, neurological AI seeking 510(k) clearance or De Novo designation should be required to demonstrate sensitivity and specificity, not just aggregate accuracy, stratified by race, ethnicity, sex, age, and socioeconomic status across a minimum sample size per subgroup. A diagnostic tool that achieves 95 percent overall accuracy but 72 percent accuracy in Indigenous patients is not a medical success. It is a racially stratified harm being deployed at clinical scale. Niazi (2026) argues that FDA sponsors submitting AI applications should be required to validate model performance across racial, ethnic, sex, and age subgroups aligned with diversity enrollment goals, a recommendation that has yet to become enforceable policy.
The third component is community-anchored site incentivization. Federated learning only produces equitable models if the sites contributing data are themselves demographically diverse. FEA would require that a certified proportion of model training weight derive from sites serving underrepresented populations, with NIH and CMS reimbursement incentives for qualifying community health organizations to establish the neuroimaging infrastructure required to participate. This is not a token gesture. ADNI’s diversity taskforce demonstrated that culturally informed, community-engaged outreach produced a 268 percent increase in the monthly enrollment rate of Black and Latinx participants, proof that inclusive participation is achievable when the institutional architecture supports it (Okonkwo et al., 2024). Together, these three components form a system rather than a checklist. Federated learning addresses the privacy barrier to diverse data. Mandatory disaggregated certification creates the regulatory incentive to close performance gaps. Community-anchored incentivization ensures that diverse sites are resourced to participate. Each component reinforces the others; none is sufficient alone.
Artificial intelligence has genuine transformative potential in neurology: detecting neurodegeneration years before symptoms emerge, extending specialist-level care to underserved communities, personalizing treatment pathways. But that potential will remain unrealized, or worse, actively harmful, if the field continues treating demographic representation as an afterthought rather than a design requirement. The brain is the organ of identity, memory, and selfhood. Diagnostic tools that systematically fail to see certain patients clearly are not merely technically inadequate. They are ethically indefensible. Federated Equity Architecture is not a perfect solution; it is an achievable one. The deeper question it forces us to answer is not technological. It is moral: whose brains do we believe are worth understanding?
References
Barnes, L. L., & Bennett, D. A. (2014). Underrepresentation of African-Americans in Alzheimer’s trials: A call for affirmative action. Frontiers in Aging Neuroscience, 6, 133. https://doi.org/10.3389/fnagi.2014.00133
Bzdok, D., & Ioannidis, J. P. A. (2023). Confronting racially exclusionary practices in the acquisition and analyses of neuroimaging data. Nature Neuroscience, 26(1), 4–11. https://doi.org/10.1038/s41593-022-01218-y
Cano, I., Vaca-Palomares, I., & Fernandez-Ruiz, J. (2024). Brain morphological variability between whites and African Americans: The importance of racial identity in brain imaging research. Frontiers in Integrative Neuroscience, 17, 1027382. https://doi.org/10.3389/fnint.2023.1027382
Daneshjou, R., Smith, M. P., Sun, M. D., Rotemberg, V., & Zou, J. (2022). Disparities in dermatology AI performance on a diverse, curated clinical image set. Science Advances, 8(32), eabq6147. https://doi.org/10.1126/sciadv.abq6147
Dinsdale, N. K., Jenkinson, M., & Namburete, A. I. L. (2022). FedHarmony: Unlearning scanner bias with distributed data. Lecture Notes in Computer Science: Medical Image Computing and Computer Assisted Intervention – MICCAI 2022, 13435, 34–44. https://doi.org/10.1007/978-3-031-16443-9_4
Li, J., Bzdok, D., Chen, J., Tam, A., Ooi, L. Q. R., Holmes, A. J., Ge, T., Patil, K. R., Jabbi, M., Eickhoff, S. B., Yeo, B. T. T., & Genon, S. (2022). Cross-ethnicity/race generalization failure of behavioral prediction from resting-state functional connectivity. Science Advances, 8(11), eabj1812. https://doi.org/10.1126/sciadv.abj1812
Li, X., Gu, Y., Dvornek, N., Staib, L., Ventola, P., & Duncan, J. S. (2020). Multi-site fMRI analysis using privacy-preserving federated learning and domain adaptation: ABIDE results. Medical Image Analysis, 65, 101765. https://doi.org/10.1016/j.media.2020.101765
Niazi, S. K. (2026). A critical review of the FDA’s draft guidance on artificial intelligence in drug and biological product regulation. Journal of Chemistry, 2026, 5202999. https://doi.org/10.1155/joch/5202999
Okonkwo, O. C., Whittle, M. T., Ashford, M. T., Raman, R., Rivera Mindt, M., & Weiner, M. W. (2024). A protocol for the inclusion of minoritized persons in Alzheimer disease research from the ADNI3 Diversity Taskforce. JAMA Network Open, 7(8), e2428308. https://doi.org/10.1001/jamanetworkopen.2024.28308
Ong, C. S., Bhatt, D. L., Khera, R., & Krumholz, H. M. (2024). Health disparities and reporting gaps in artificial intelligence (AI) enabled medical devices: A scoping review of 692 U.S. Food and Drug Administration (FDA) approvals. npj Digital Medicine, 7, 265. https://doi.org/10.1038/s41746-024-01270-x
Raman, R., Ashford, M. T., Miller, G., Donohue, M. C., Okonkwo, O. C., Rivera Mindt, M., Nosheny, R. L., Coker, G. A., Petersen, R. C., Aisen, P. S., & Weiner, M. W. (2023). Screening and enrollment of underrepresented ethnocultural and educational populations in the Alzheimer’s Disease Neuroimaging Initiative (ADNI). Alzheimer’s & Dementia, 19(2), 717–726. https://doi.org/10.1002/alz.12756
Rezaei, M., Samsami, M., Mohammadi, M., & Karimzadeh, F. (2024). Artificial intelligence in neuroimaging: Opportunities and ethical challenges. NeuroImage Reports, 4(3), 100213. https://doi.org/10.1016/j.ynirp.2024.100213
